Dear xx
Thank you for getting back to me.
The debate I am suggesting would primarily focus on evidence-based decision-making. There are of course massive ethical issues arising from New Zealand’s ruthless policies to stop the spread of SARS-CoV-2, but my biggest concern is the government’s failure to assess the evidence objectively, and its psychological blindness to alternative strategies.
At the start of the ‘pandemic’ I wrote a book, The Case for Democracy in the Covid 19 pandemic (https://uk.sagepub.com/en-gb/eur/the-case-for-democracy-in-the-covid-19-pandemic/book275656). Its description covers many issues. These remain relevant almost two years on:
“One moment life was normal, the next, governments around the world were imposing radical lockdowns of their populations. But why were decision-makers so readily ignoring centuries of hard-won civil freedoms? Where was the discussion of ethics and human rights? Why were we so easily controlled and why were our controllers so willing to do it?
In The Case for Democracy, David Seedhouse explores the psychological biases; distorted risk perceptions; frenetic journalism; the disputed science; the narrow focus of 'experts'; value judgements dressed up as truths; propaganda; the invisibility of ethics; and the alarming irrelevance of inclusive democracy that have been features of governmental responses to the covid-19 pandemic.
Seedhouse argues that the chaotic governmental response to Coronavirus, with no attempt to include the public, is the perfect argument for an extensive, participatory democracy; a democracy that demonstrates practical decision making by listening to everyone’s knowledge and expertise.”
NATURAL IMMUNITY
Note also that I refer to the ‘pandemic’ in quotes since it can be called a pandemic only because the World Health Organisation changed its definition in 2009:
“Since 2003, the top of the WHO Pandemic Preparedness homepage has contained the following statement: “An influenza pandemic occurs when a new influenza virus appears against which the human population has no immunity, resulting in several simultaneous epidemics worldwide with enormous numbers of deaths and illness.” However, on 4 May 2009, scarcely one month before the H1N1 pandemic was declared, the web page was altered in response to a query from a CNN reporter. The phrase “enormous numbers of deaths and illness” had been removed and the revised web page simply read as follows: “An influenza pandemic may occur when a new influenza virus appears against which the human population has no immunity.” https://www.who.int/bulletin/volumes/89/7/11-086173.pdf
On the 2009 definition there is no pandemic. Ignoring the interpretation of ‘enormous’ which will always be controversial, it is just not true that there is no natural immunity to SARS-CoV-2. This article lists thirty scientific studies which show this beyond any doubt: https://brownstone.org/articles/natural-immunity-and-covid-19-twenty-nine-scientific-studies-to-share-with-employers-health-officials-and-politicians/amp/
“These studies demonstrate what was and is already known: natural immunity for a SARS-type virus is robust, long-lasting, and broadly effective even in the case of mutations, generally more so than vaccines. In fact, a major contribution of 20th-century science has been to expand upon and further elucidate this principle that has been known since the ancient world.”
These studies falsify your belief that “getting people vaccinated … is the most effective and sustainable way to protect a population against an infectious disease like covid”.
The Brownstone document has recently been further updated. It offers a comprehensive library list of 150 of the highest-quality, complete, most robust scientific studies and evidence reports/position statements on natural immunity: https://brownstone.org/articles/79-research-studies-affirm-naturally-acquired-immunity-to-covid-19-documented-linked-and-quoted/
Here is just one example: “Exposure to common cold coronaviruses can teach the immune system to recognize SARS-CoV-2” – because of T-cell memory: https://www.lji.org/news-events/news/post/exposure-to-common-cold-coronaviruses-can-teach-the-immune-system-to-recognize-sars-cov-2/. T-cell memory is a virology fundamental: https://teachmephysiology.com/immune-system/adaptive-immune-system/t-cell-memory/
If you and your colleagues are unaware of this meta-analysis I recommend you give it urgent attention. It says in sum:
“… existing immunity should be assessed before any vaccination, via an accurate, dependable, and reliable antibody test (or T cell immunity test) or be based on documentation of prior infection (a previous positive PCR or antigen test). Such would be evidence of immunity that is equal to that of vaccination and the immunity should be provided the same societal status as any vaccine-induced immunity. This will function to mitigate the societal anxiety with these forced vaccine mandates and societal upheaval due to job loss, denial of societal privileges etc. Tearing apart the vaccinated and the unvaccinated in a society, separating them, is not medically or scientifically supportable.”
I would add ‘not ethically supportable’ to this statement.
WHY VACCINATE?
Given this, the practical value of continuing a ‘vaccination’ programme is highly questionable. Traditional vaccines consist of entire pathogens that have been killed or weakened so that they cannot cause disease whereas ‘Covid vaccines’ manipulate the genes of the recipients and do not produce a full immune response.
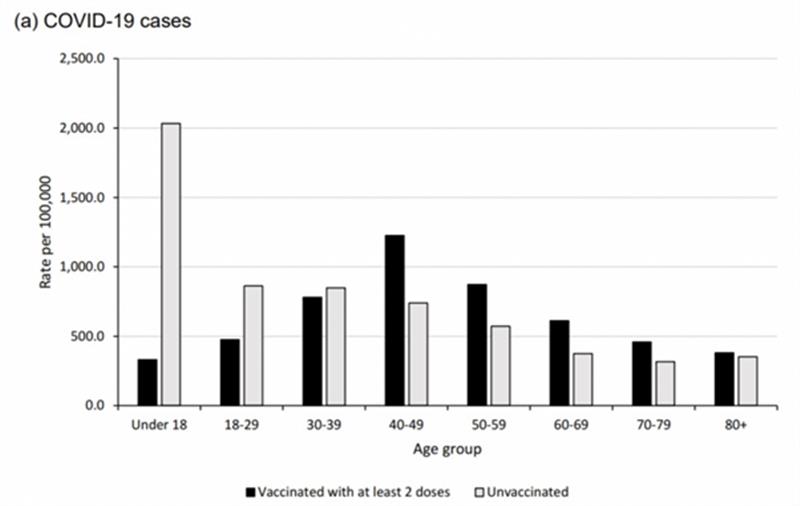
The latest science tells us that the ‘Covid vaccines’ do little to prevent infection or transmission (and so cannot prevent or stop outbreaks) but they do reduce severe disease and death in the vaccinated, albeit not by as much as was originally claimed: https://www.gov.uk/government/publications/investigation-of-novel-sars-cov-2-variant-variant-of-concern-20201201
But even this protection wanes:
https://www.gov.uk/government/publications/covid-19-vaccine-weekly-surveillance-reports
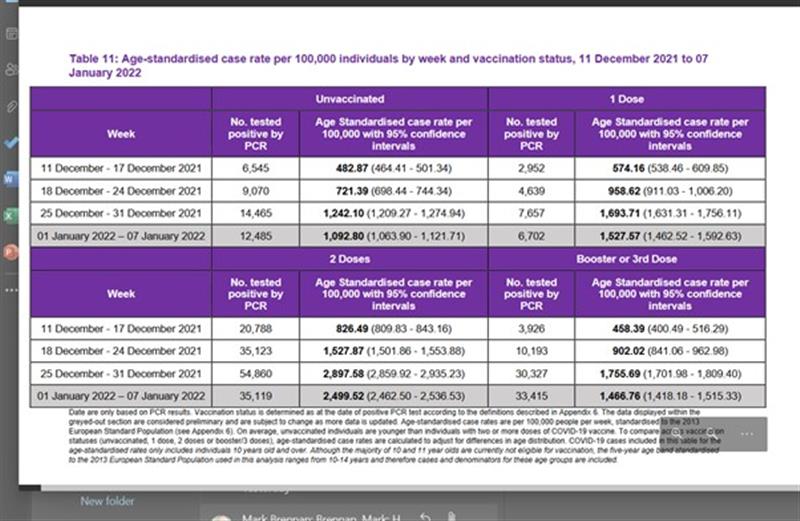
https://publichealthscotland.scot/media/11089/22-01-12-covid19-winter_publication_report.pdf
These latter data show that those who are vaccinated are 2 and a half times more likely to be infected than those who are not.
Of course these figures are open to interpretation, but it is clear that:
“As Sunetra Gupta, Professor of Theoretical Epidemiology at Oxford University, notes, vaccines are best understood as part of focused protection, providing some additional protection against serious disease and death for those at high risk. They should not be used for something they are evidently unsuited for: the effort to reduce infections to permanently low levels via a vaccine-induced herd immunity. She writes:
Vaccines typically do not outperform natural immunity, so it should come as no surprise that Covid vaccines do not offer long-term protection against infection. At the same time, we can be confident that they will continue to work well to prevent severe clinical outcomes. The role of these vaccines is to offer protection to the clinically vulnerable; to foist them upon those who are at negligible risk in the hope of augmenting herd immunity is illogical…
For there to be the collective benefit of herd immunity, the booster would have to provide life-long protection against infection – unless we are willing to accept repeated mass vaccination into the foreseeable future. Aside from being a colossal diversion of limited resources, that would open the door to a permanent state of lockdown as we lurch from one booster campaign to the next.
Instead, we should acknowledge that “the vaccines have already brought focused protection to those who needed it in the U.K. and that now the best course of action is to rely on natural immunity to maintain and consolidate a normal state of living with this virus”.” https://dailysceptic.org/2021/09/03/the-push-for-vaccination-of-children-and-vaccine-boosters-despite-the-lack-of-evidence-they-prevent-infection-or-transmission-is-approaching-a-religious-mania/
PSYCHOLOGICAL FIXATIONS
At the start of the ‘pandemic’ it briefly made sense to close the international borders in case the illness was worse than expected, but this has made less and less sense as time has passed, evidence has accumulated, and more treatments are available for people who need them (though for the vast majority infection is mild or not even noticeable).
But the government – or rather its small team of advisers, of which you are one – has fallen prey to an array of psychological biases, for example, confirmation bias, attentional bias, illusion of control bias, groupthink and the amplification of risk out of any reasonable proportion. This has caused a blindness to anything other than the official ‘hardline’, and a stubborn inability to carry out a proper cost-benefit analysis incorporating factors other than disease. Under the powerful influence of this obsession the only thing that matters is controlling the virus:
“'The country's surging Covid cases are the priority for the Government - not the illegal actions of protesters at Parliament, Prime Minister Jacinda Ardern told reporters in Rotorua earlier today.
The focus needed to be on the 'growing pandemic and keeping people safe,' Ardern said.
'What is happening there is illegal,' she said of the protesters.
'I don't expect it to change quickly, we're all prepared for it to take some time but despite that, it will not change our force.
'We have a duty to all New Zealanders to focus on the pandemic.''
In the same article:
“Sixty-three people are in hospital with Covid-19 - none in intensive care.” https://www.nzherald.co.nz/nz/covid-19-omicron-outbreak-record-1573-new-cases-jacinda-ardern-says-infections-her-concern-not-illegal-protest/T5CEVXKLRSD5HKPRQW3OFMR32M/
The Prime Minister’s position just doesn’t make sense on any level.
ETHICS
You say that you are not the right person to be ‘debating the rights and wrongs of the policies from an ethical perspective’, but this is part of the problem. Public health interventions are not automatically ethical, in fact what has happened in NZ has been extraordinarily unethical on any conventional understanding of ethics. The fact that this is not obvious demonstrates the power of the psychological delusions you and your fellow decision-makers are under.
If you don't feel able to debate the ethical rights and wrongs of population-wide policies then, respectfully, you really shouldn't be making them.
Very briefly:
- New Zealand citizens have been prevented from coming home, despite our Bill of Rights which is supposed to protect our fundamental freedoms.
- The scientific evidence that vaccines don’t prevent infection or transmission has been ignored
- The scientific evidence that masks don’t prevent transmission has been ignored
- A massive propaganda campaign has been undertaken to persuade as many people as possible to be vaccinated, despite the growing evidence the ‘vaccines’ are ineffective at protecting others, and carry significant risks of adverse events to the individual: https://dailysceptic.org/2022/01/18/vaccine-safety-update-23/
- Vaccine passports and mandates have been introduced effectively rendering NZ a two-tier society, impeding normal daily activities for all New Zealanders who do not wish to receive experimental injections: https://drive.google.com/file/d/1EhH3qggKFY68Y4MsWGkUIRHbbcNxX31-/view. Even if the ‘vaccines’ were effective in stopping transmission it is fundamentally wrong to force people to accept them. In the Western world until now, the principles of informed consent and bodily autonomy were sacrosanct. There is no practical or moral reason why this should not remain the case.
- Children who are at virtually no risk from SARS-CoV-2 have been coerced into accepting ‘vaccines’ that not only can do them no good but may cause harm (we just don’t know for sure). There is no ethical or practical reason to ‘vaccinate’ children.
- Children who are at virtually no risk from SARS-CoV-2 have been coerced into accepting vaccines on the false premise that by doing so they will protect others, but this is not and never has been the point of vaccines. Vaccines are designed to protect the individual, not society. And we now know from the science that vaccinating children protects no-one.
THE LIMITS OF PUBLIC HEALTH
It is easily demonstrated that public health is not an imperative. If it is acceptable to coerce people into accepting vaccines in the interest of protecting others – which is the only conceivable reason to do so – then it must also be acceptable to coerce people to diet, to exercise, to stop smoking, to cycle rather than drive, not to have sex with strangers and so on. But it isn’t acceptable because we respect people’s rights to make their own choices in a free and liberal society, unless their choices will directly harm other individuals.
WHAT SHOULD BE DONE
- New Zealand decision-makers remain so obsessed with the virus that all other considerations pale into insignificance. This unhealthy phenomenon could be swiftly addressed by inviting experts from various disciplines to meet virtually in a summit conference to advise New Zealand on how best to create a balanced approach that allows the normal functioning of society while protecting vulnerable people.
- From now on public health decisions should be made by experts from a range of disciplines including law, economics, psychology and ethics, not just public health and related disciplines. Members of the public must also be involved and must have meaningful input.
- New Zealand citizens must be allowed to enter and leave the country freely.
- The Bill of Rights must be respected and given proper legal force.
- Vaccine mandates and passports must be immediately rescinded.
- Since SARS-CoV-2 seems to be progressively weakening – the omicron variant is milder than the delta variant – New Zealanders should be allowed to live entirely normally, which would have the added benefit of promoting natural immunity.
- The government should no longer cite New Zealand as an example of success ‘against Covid’. Rather it should admit that mistakes were made, in good faith, and that policy will change in line with the evidence with immediate effect.
It is proposed that this reply should be sent and also published as an Open Letter